




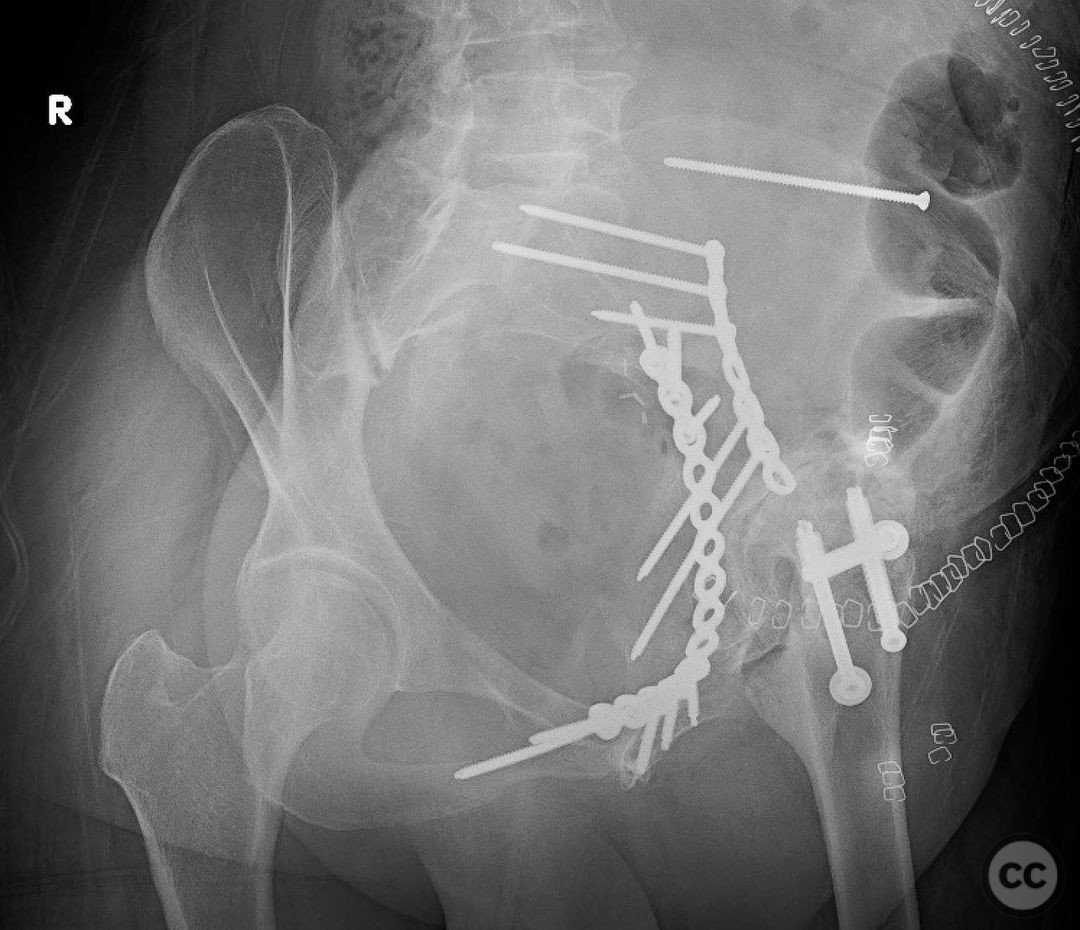
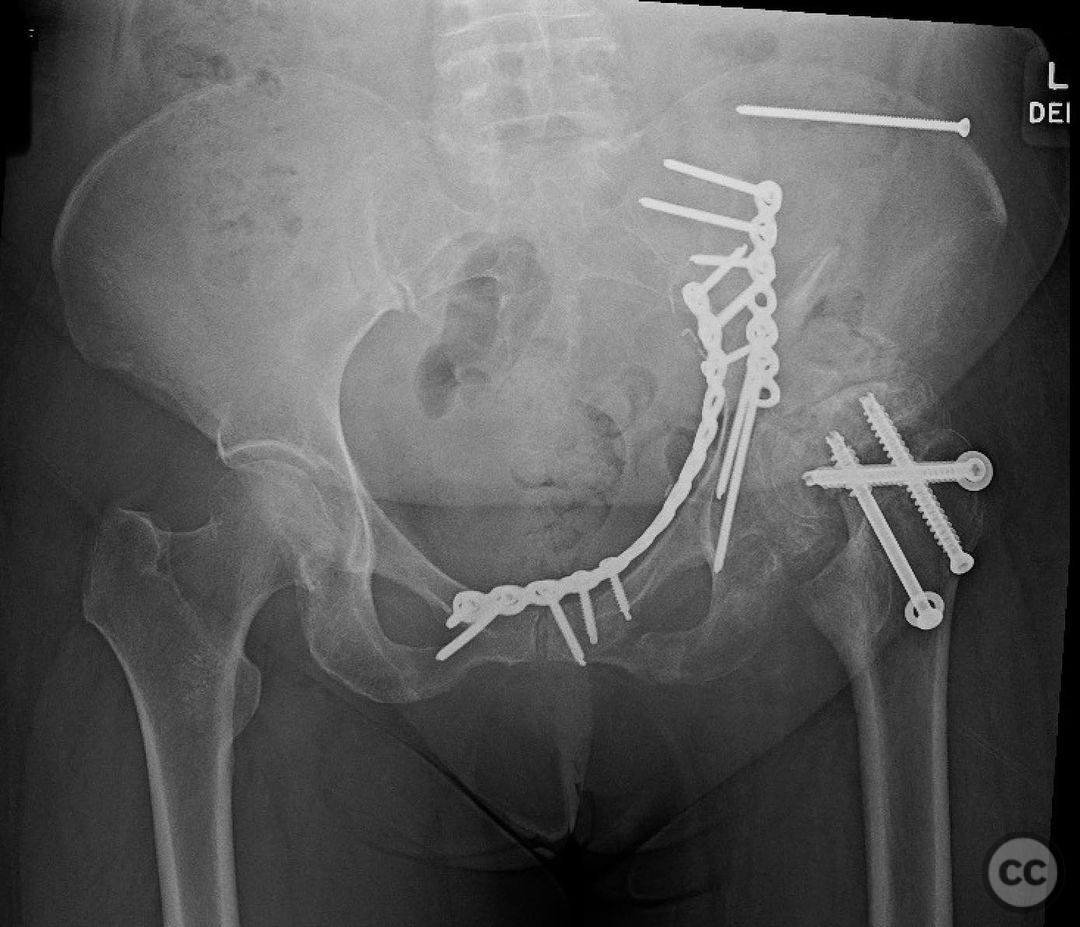
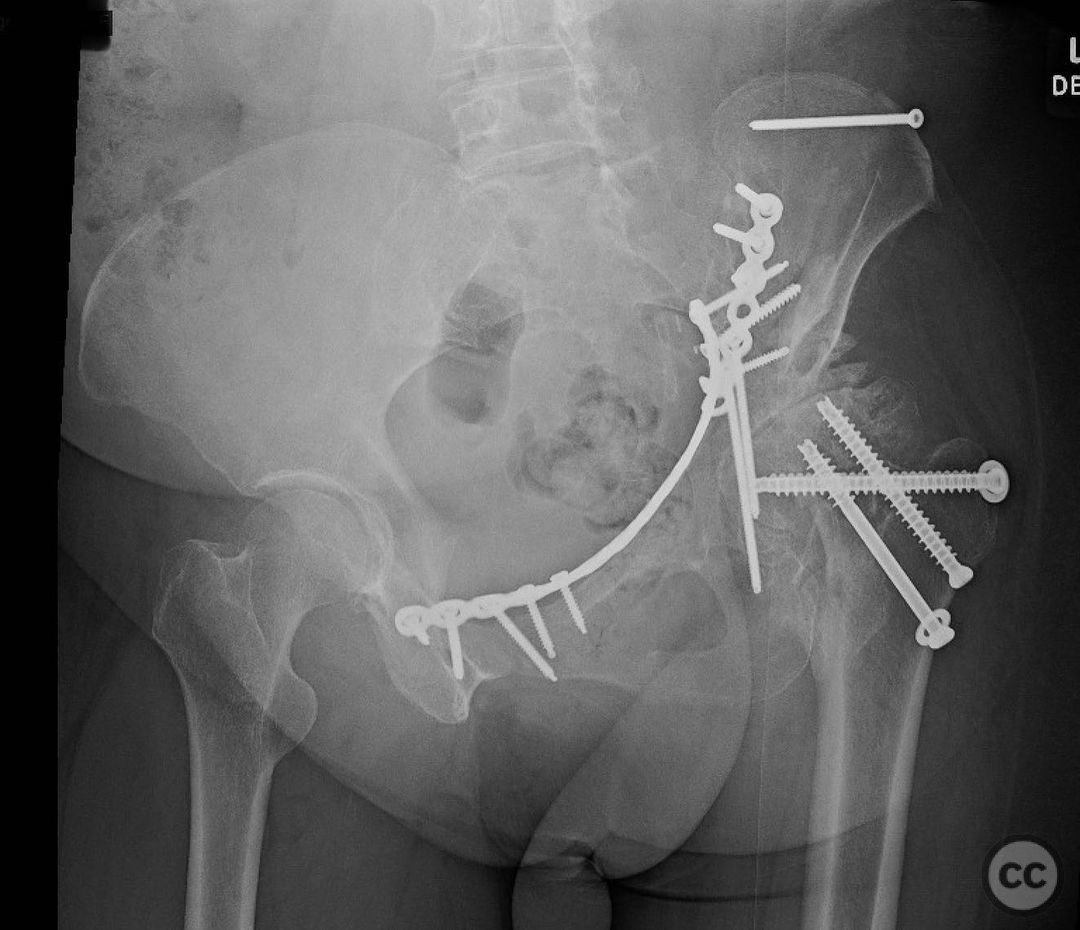
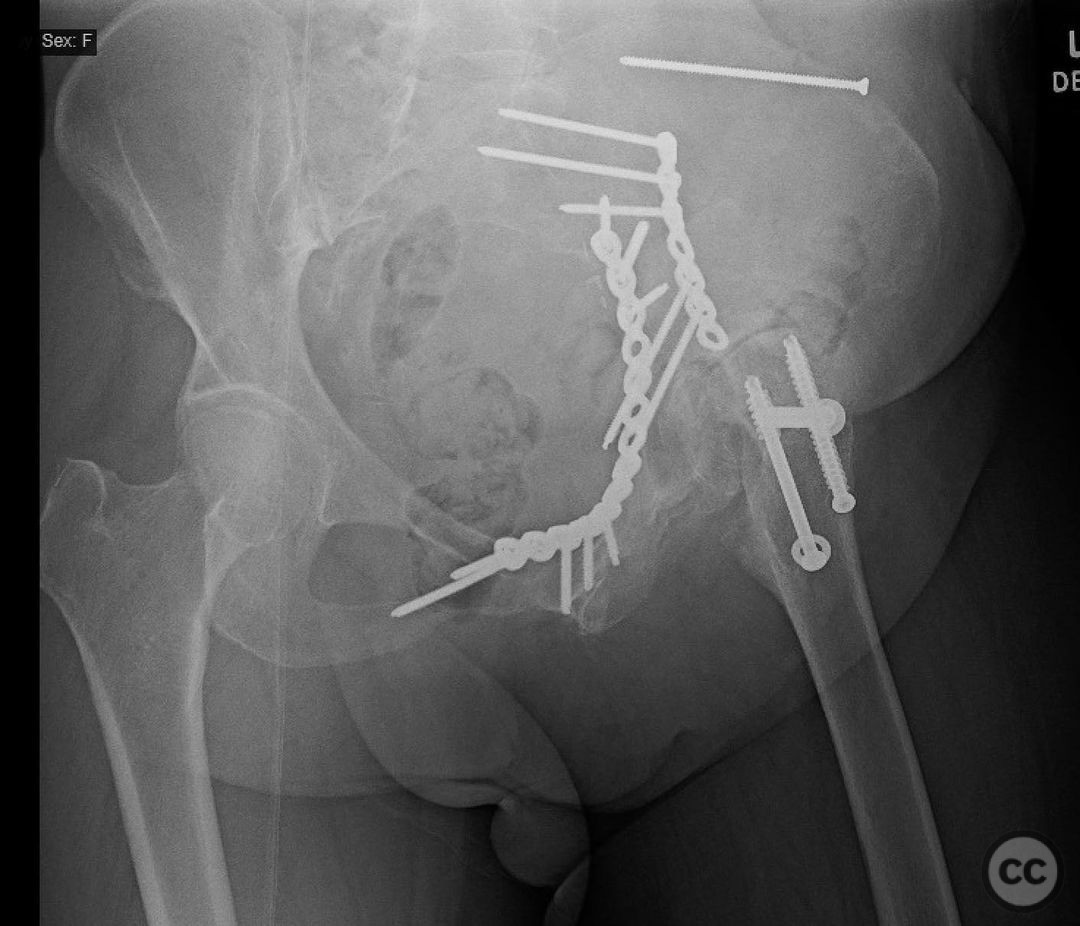
Associated both column acetabular fracture and a femoral neck fracture with OA
Score and Comment on this Case
Clinical Details
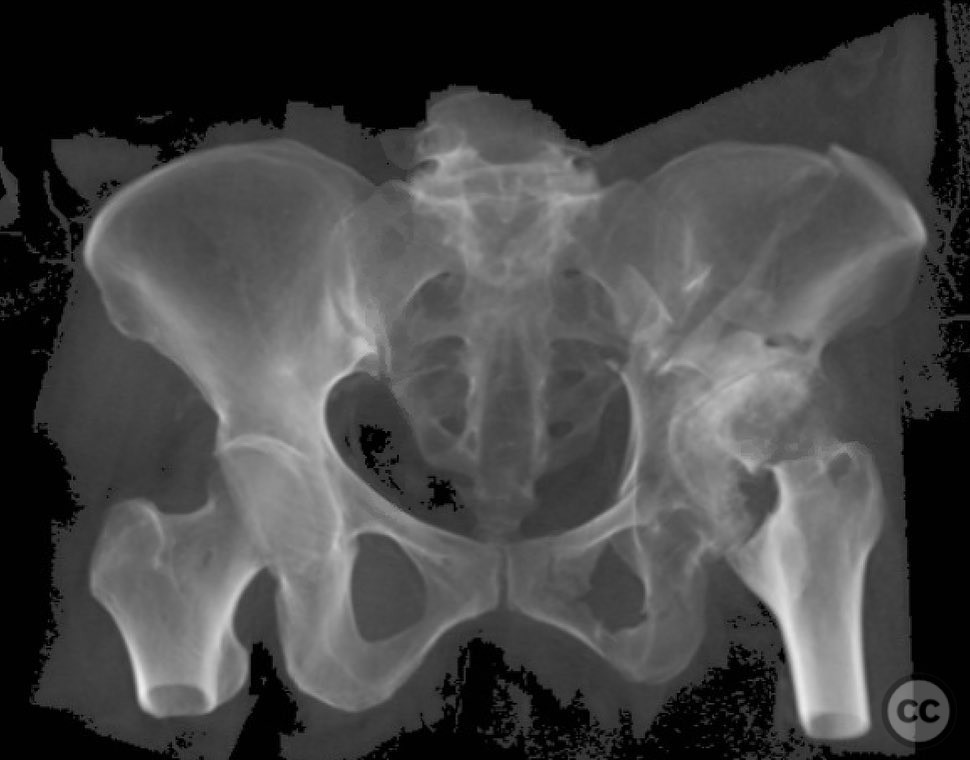
Clinical and radiological findings: This is a 69yo woman who crashed her motorcycle. She’s got advanced OA and now an extra-articular (but just barely) associated both column acetabular fracture and a femoral neck fracture. Prior to her accident she has no hip pain. She’s very active, and while her hip is a bit stiff on that side it doesn’t limit her and it never hurts. She knows she has a history of dysplasia and subsequent avn. She saw a joints surgeon 4 years ago but only at the recommendation of her pcp after seeing some X-rays after a routine dexa scan. Because she had no pain or limitations she deferred the idea of a tha indefinitely. So bottom line- pre-injury she is happy with her hip.
Preoperative Plan
Planning remarks:
Surgical Discussion
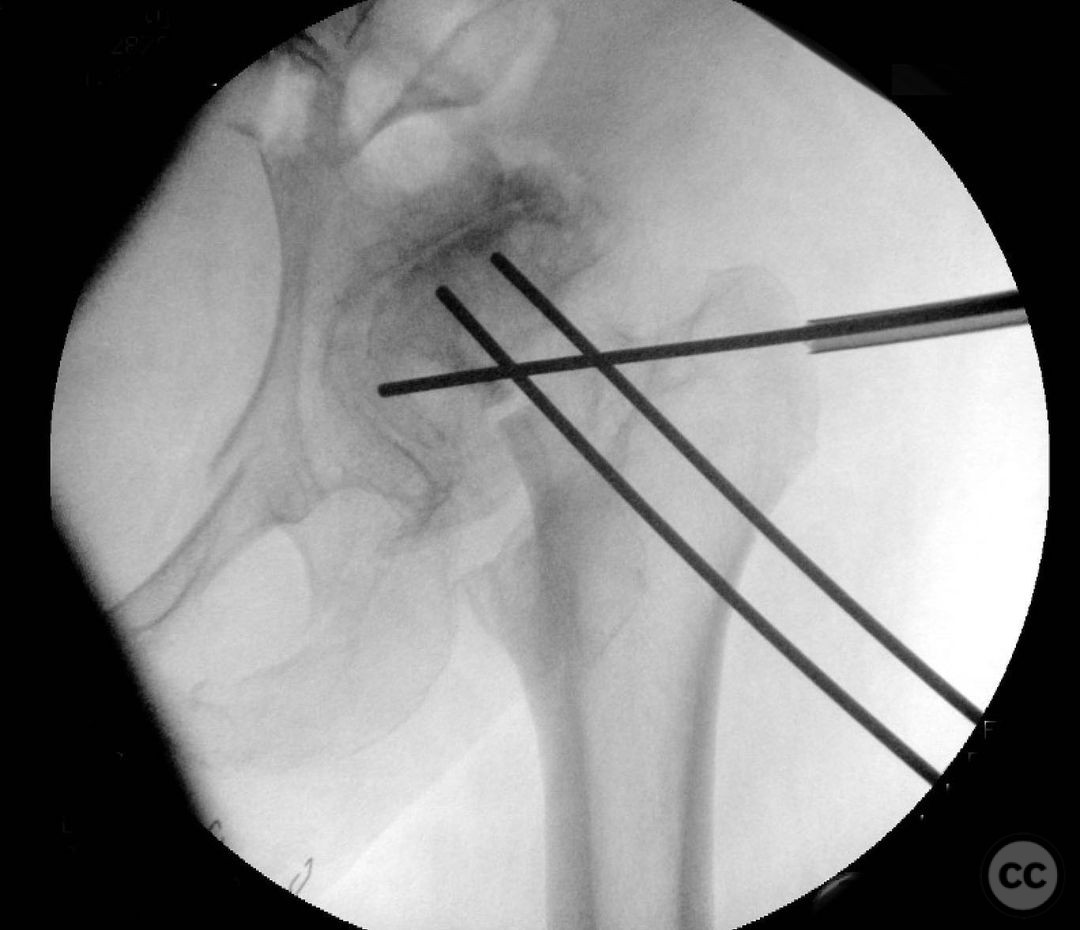
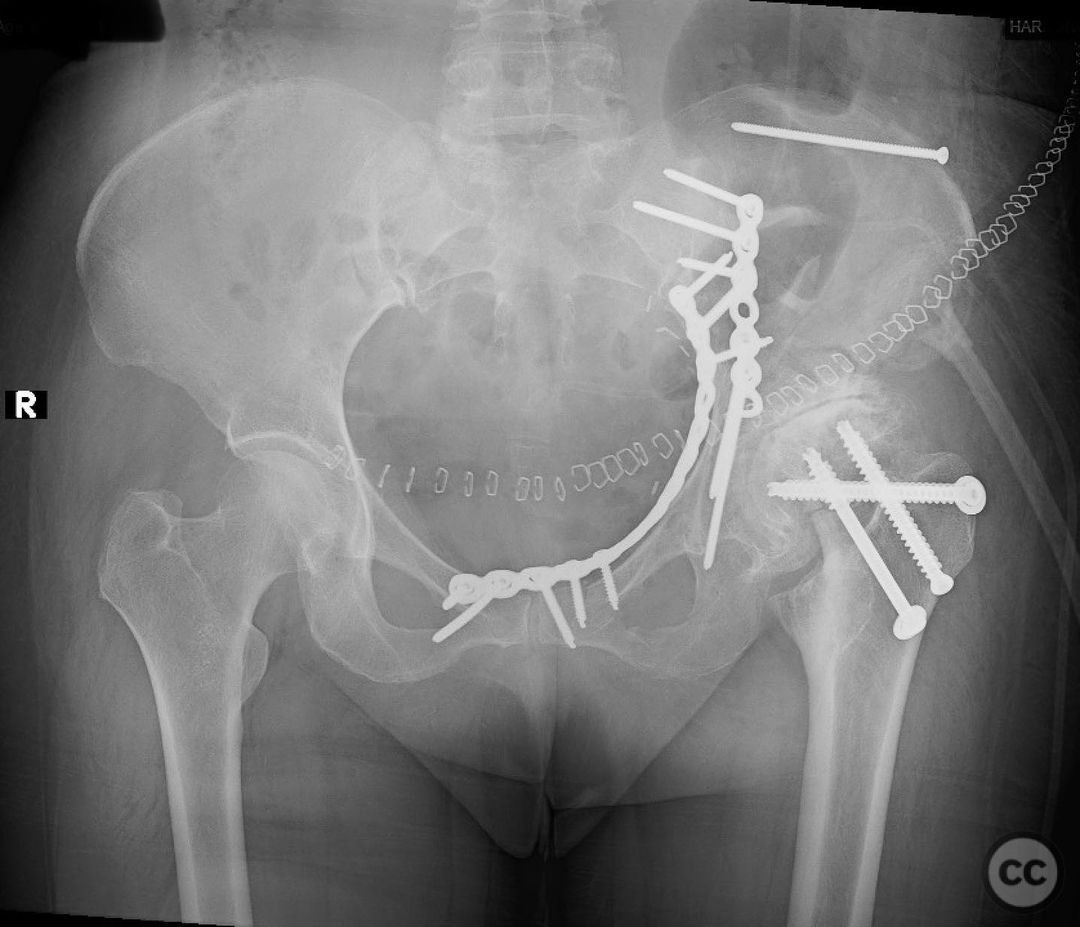
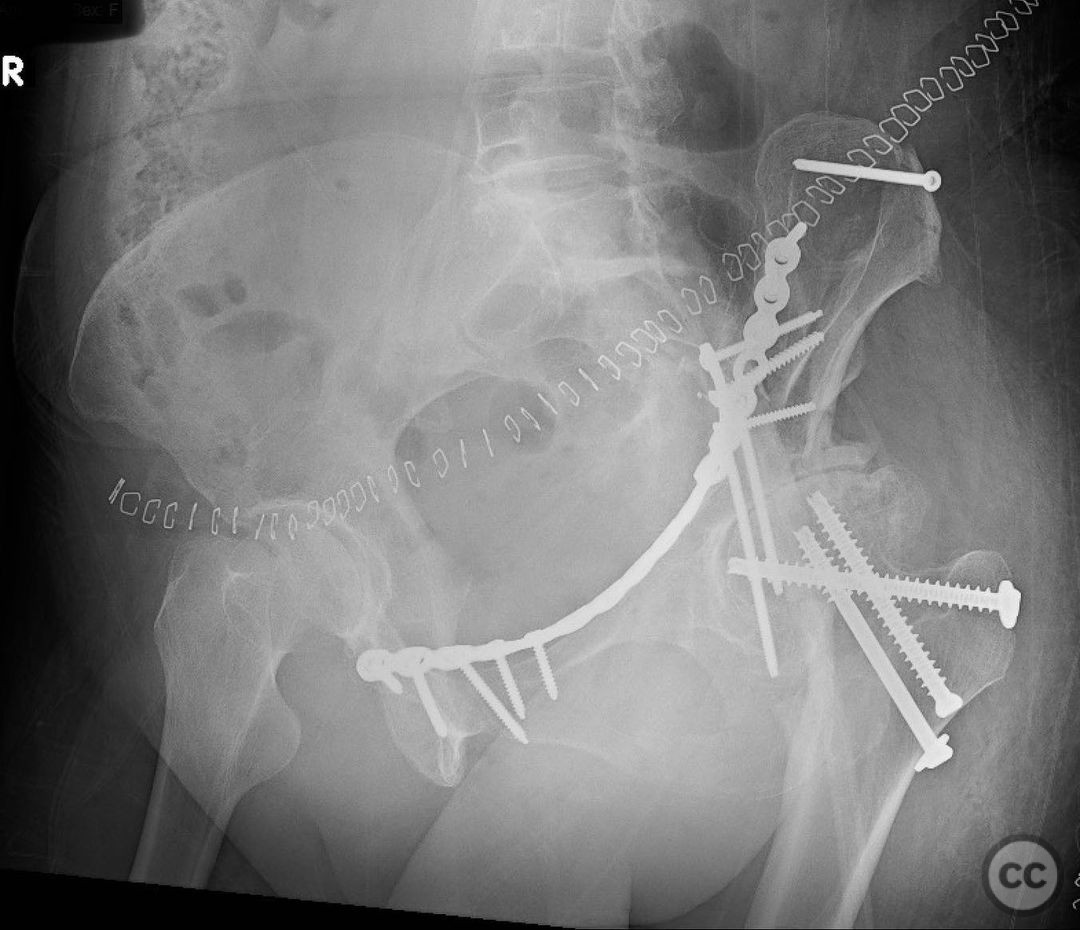
Operative remarks:A THA would be the treatment of choice in a patient of this age with a femoral neck fracture in the setting of OA, but of course we have this acetabular fracture to deal with- in some cases, acute ORIF + THA (stabilize the columns, get a stable and well fixed cup in), but not in this case. The posterior column is segmental with a free sciatic buttress, and the anterior column is definitely not going to be stable enough acutely to help. Also, some surgeons are staying from acute ORIF + THA when multiple approaches are required due to the risk of infection. So that leaves us with 2 options 1) fix them both and THA at 6-8 weeks or 2) just fix it and see how she does. A big part of this decision is how the patient was pre-injury. If they were miserable, a conversion would be a pretty easy answer. But as in this case, the patient was doing well enough that she really didn’t want a THA. She is now almost 6 months out, healed, ambulatory, and doing pretty well. She’s met with a joints surgeon and is going to continue to hold off on the hip for now. My biggest worry in this case was early failure of femoral neck fracture fixation. Because her hip is so still, there is a ton of stress concentration at the neck fracture. I was 50/50 on whether the screws work, and that’s why I went with the configuration (compress, then “lock in” with pauwels screw, and pray)
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 570 times
28 Nov 2022
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2022). Associated both column acetabular fracture and a femoral neck fracture with OA. Journal of Orthopaedic Surgery and Traumatology. Case Report 8009960 Published Online Nov 28 2022.