















Impacted Distal Radius Fracture with Volar and Dorsal Rim Involvement
Score and Comment on this Case
Clinical Details
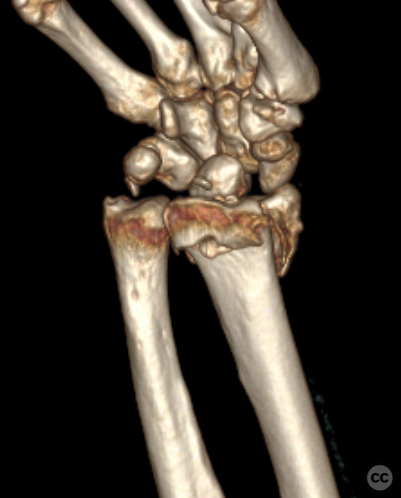
Clinical and radiological findings: A 78-year-old female sustained a ground-level fall resulting in a classic Colles' dinner-fork deformity. Initial radiographs demonstrated marked axial impaction and dorsal angulation. Computed tomography confirmed a multifragmentary fracture with volar and dorsal rim fragments, as well as a separate radial styloid fragment.
Preoperative Plan
Planning remarks: The planned surgical approach was a volar Henry's approach to the distal radius, utilizing an extended longitudinal incision over the flexor carpi radialis in an E-FCR type approach.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table, with the right arm placed on an auxiliary arm table in an atonic state. A tourniquet was applied to the proximal aspect of the ipsilateral arm.
Anatomical surgical approach: A longitudinal incision was made over the flexor carpi radialis, incorporating a zigzag pattern over the flexor crease. Subcutaneous dissection and incision of the flexor sheath overlying the FCR were performed. The FCR tendon was retracted to the ulnar side, followed by an incision of the antebrachial fascia and identification of the flexor pollicis longus (FPL), which was similarly mobilized to the ulnar side. The pronator quadratus was incised along its radial border and along the watershed zone, allowing subperiosteal elevation to expose the distal radial metaphyseal fracture.
Operative remarks:The fracture presented with marked impaction and approximately one centimeter of shortening, alongside significant dorsal angulation due to a dorsal defect zone. Mobilization of the fracture through osteotomes and debridement of dorsal callus resulted in incremental improvement in mobilization; however, complete reduction of the distal articular fragment remained challenging. Consequently, a 1.8 millimeter Kirschner wire (K-wire) was introduced into the body of the scaphoid and another 1.8 millimeter K-wire into the distal radial diaphysis. Ligamentotaxis applied over the radiocarpal ligaments facilitated excellent restoration of overall radial length. Residual dorsal angulation was corrected through "distal fragment first" plate fixation; thus, a three plus seven hole two-column distal radial plate was affixed to the distal fragment utilizing five subchondral screws. Further fine positioning of this plate on the diaphysis corrected radial translation and significantly improved radial column length. Multiplanar fluoroscopy confirmed restoration of joint geometry and absence of intra-articular hardware; tangential dorsal views verified no dorsal screw penetration into extensor compartments.
Postoperative protocol: Postoperatively, the patient was placed in a volar splint for immobilization. Early range of motion exercises were initiated at two weeks post-surgery, with gradual progression to weight-bearing activities by six weeks postoperatively.
Follow up: Not specified
Orthopaedic implants used: - 1.8 mm Kirschner wires and Hintermann K-Wire distractor - Synthes two-column distal radial plate
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 738 times
17 Jul 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Impacted Distal Radius Fracture with Volar and Dorsal Rim Involvement. Journal of Orthopaedic Surgery and Traumatology. Case Report 8127443 Published Online Jul 17 2024.