
Reverse Barton's fracture 2R3B3.1
Score and Comment on this Case
Clinical Details
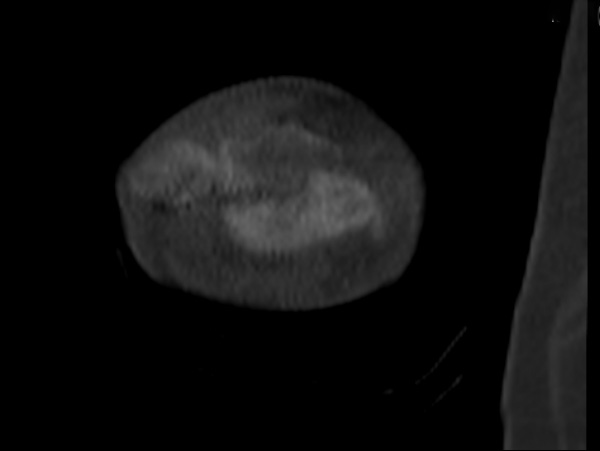
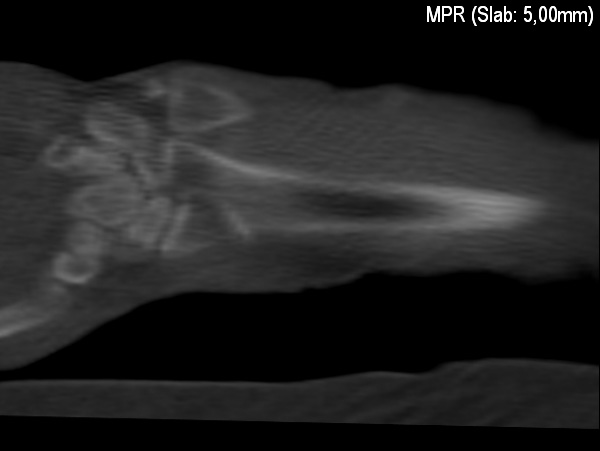
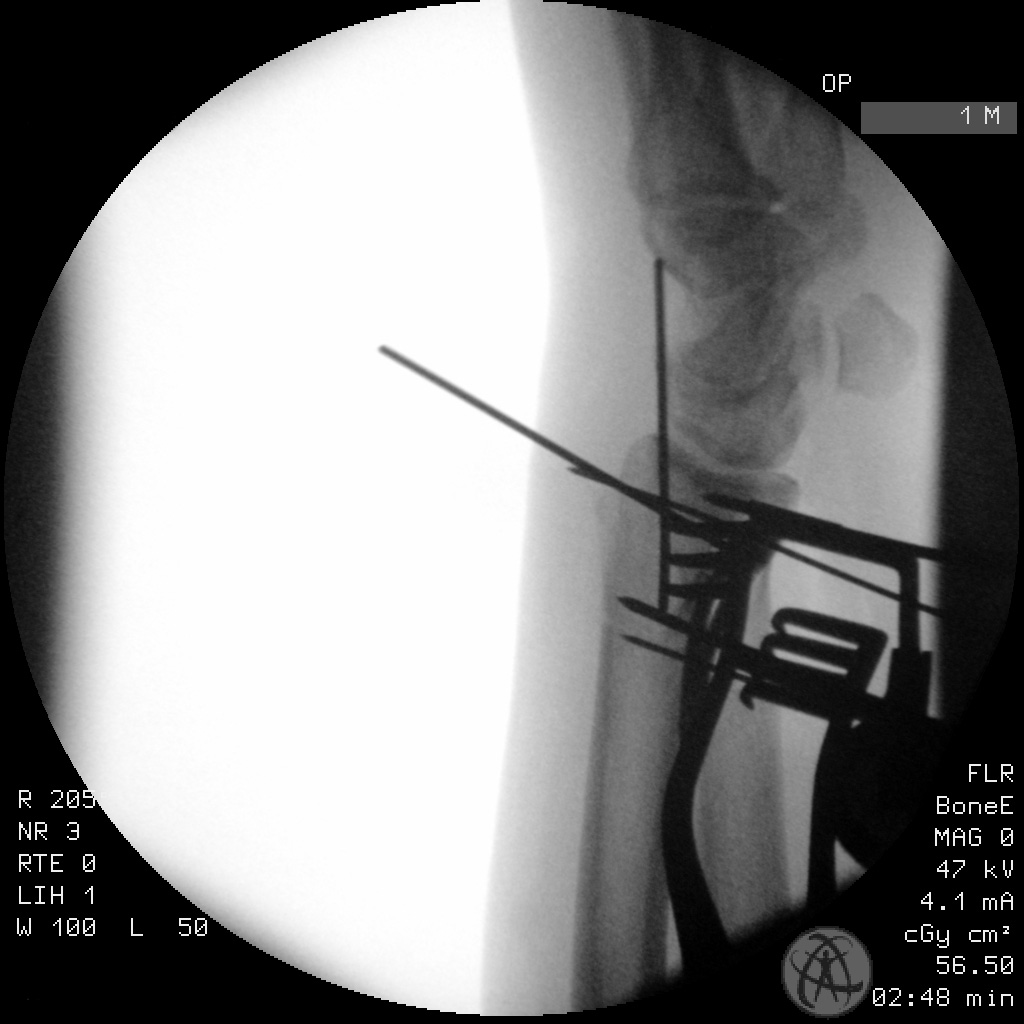
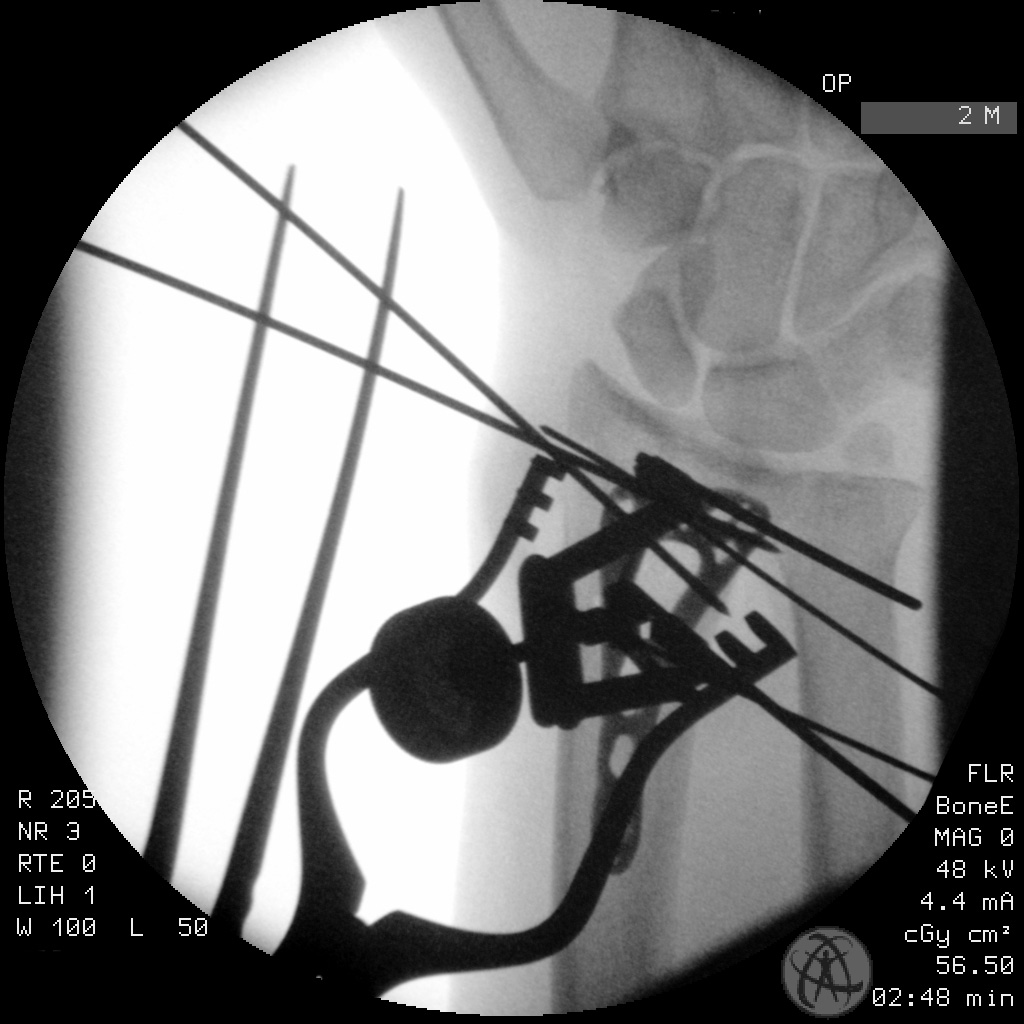
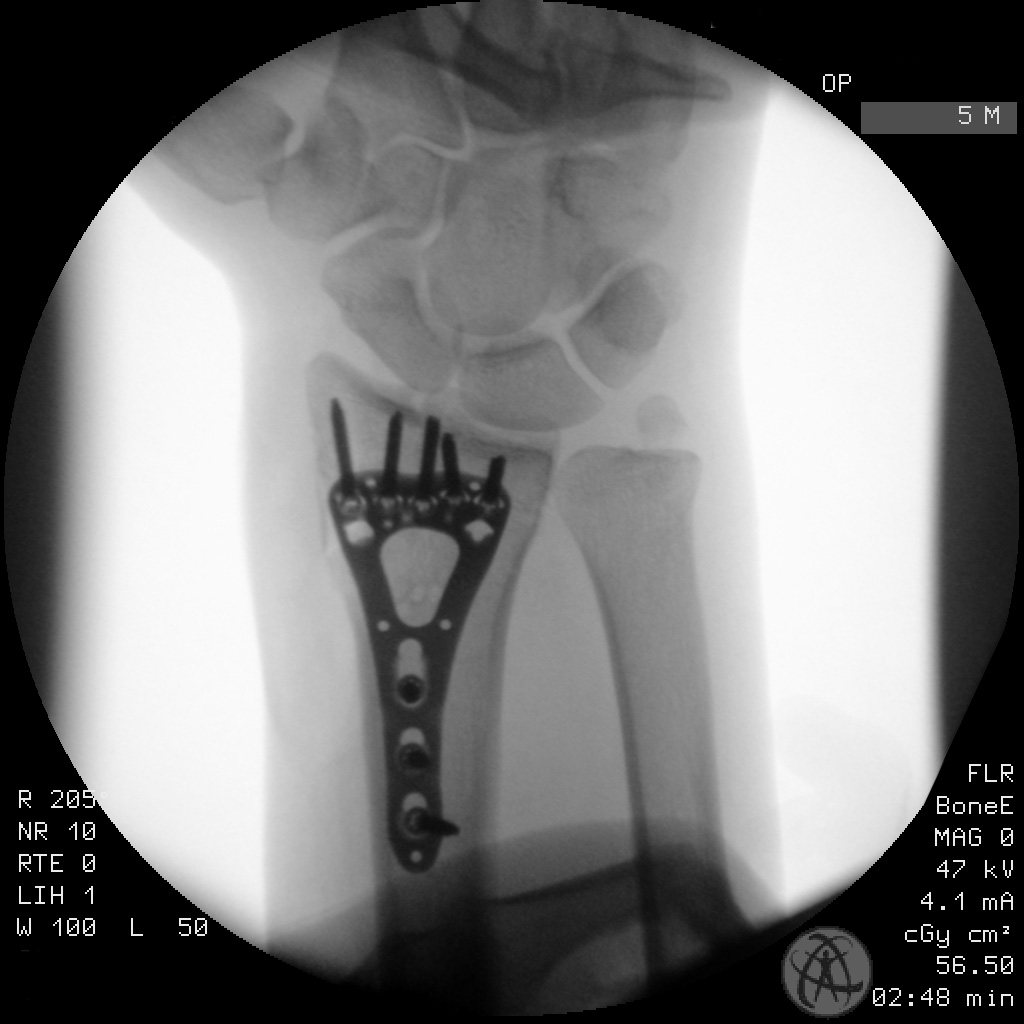
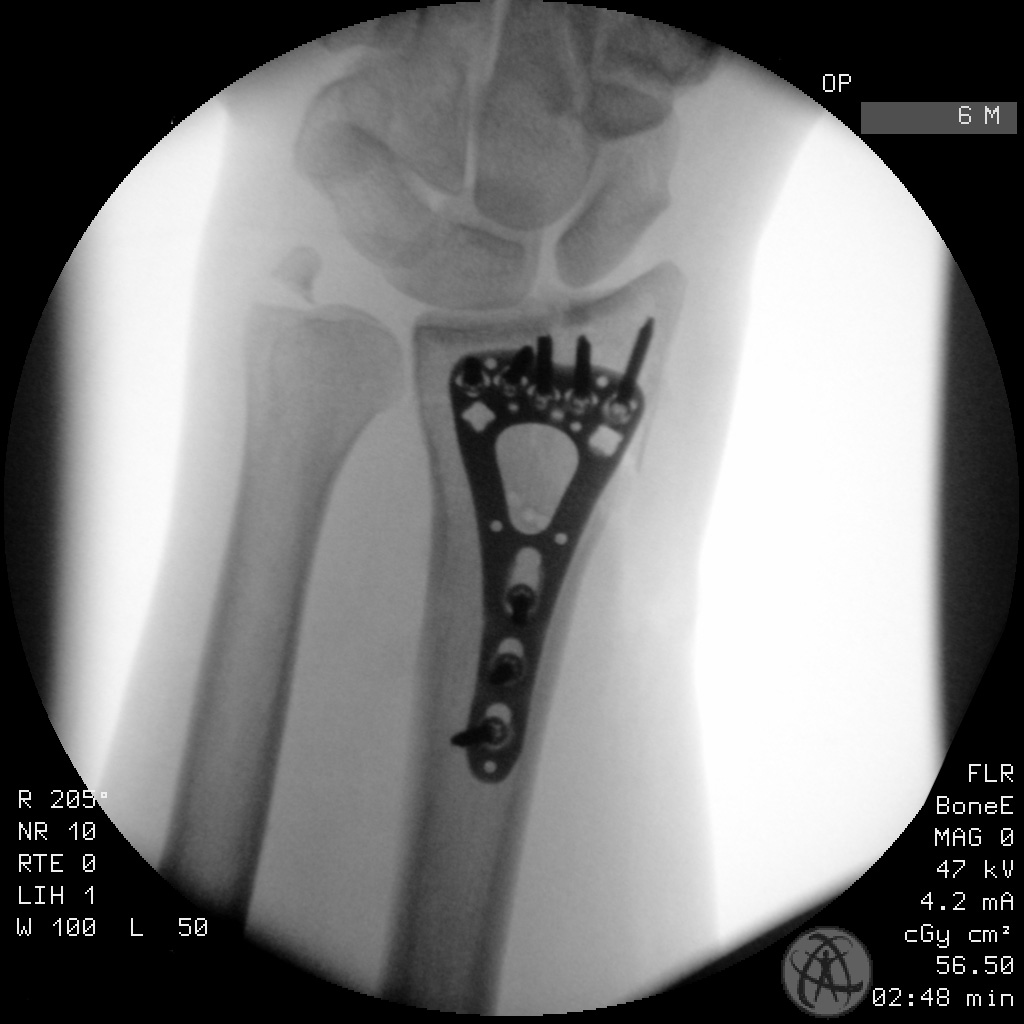
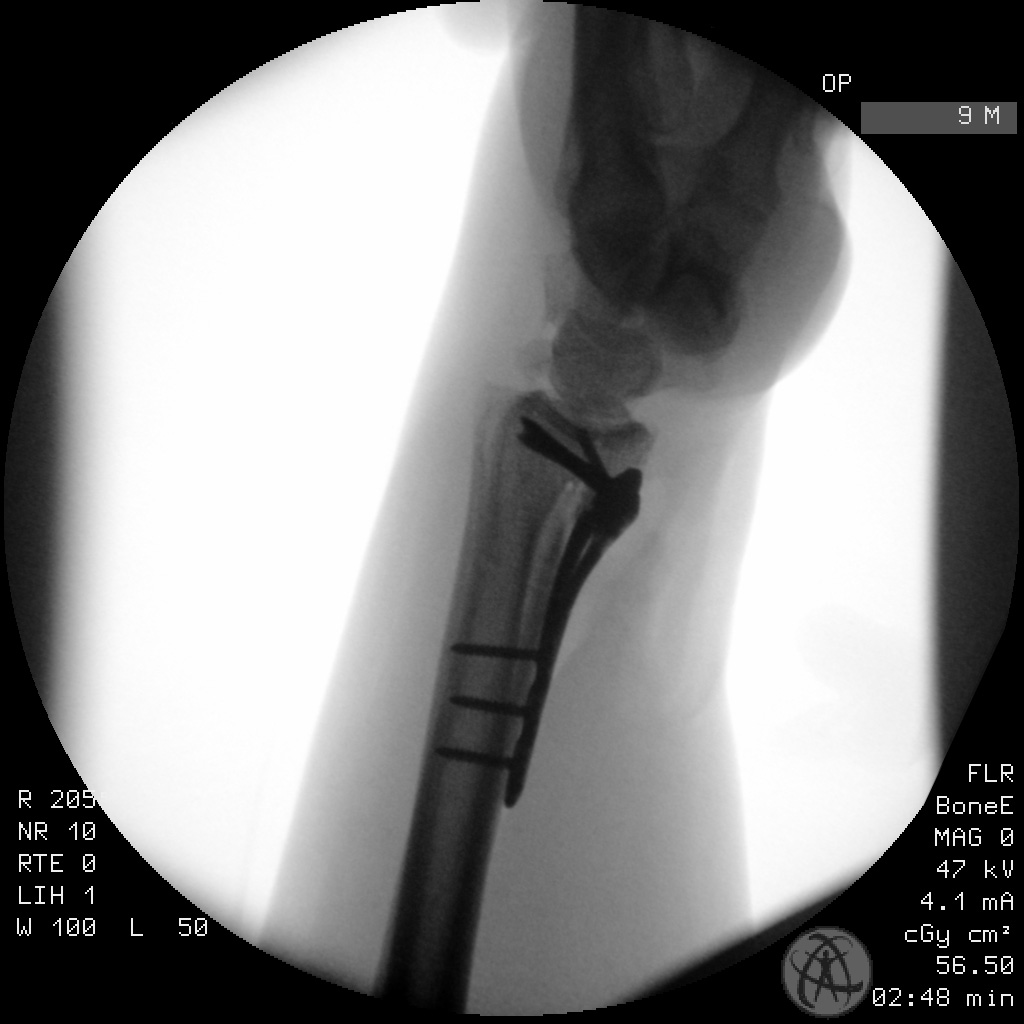
Clinical and radiological findings: This is a 47-year-old male who was involved in a motor vehicle accident. Amongst his various injuries so was this distal radius fracture/diclocation as identified in his trauma scan. Unfortunately we don’t have any plain film imaging of the wrist - only these reconstructions from the CT trauma series are available for pre-operative evaluation. The operation was a done supine with the arm on a small arm table to the side of the main operating table. A standard Henry’s approach over the FCR was utilized. Despite a complete mobilization of pronator quadratus and debridement of the fracture itself, the palmer fragment was incredibly stubborn to reduce due to the subluxation of the carpups. I employed a linear retractor with 2 K-wires to help reduce the fragment to it’s complete length restoring the continuity of the articular surface and reduce the RCJ. Whilst reduction was being maintained by the linear retractor i then temporarily fixed the reduction with the two K wires brought in from the radial styloid. Subsequently the fracture was definitively fixed with a two column distal radial locking plate. The radius plate provided excellent buttressing of this palmar fragment and held excellent joint congruity.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:This is the first radial fracture I’ve had occasion to use a K-wire based linear retractor for the reduction of a fragment. Reduction this fragment was particularly difficult due to the concominant subluxation of the carpus and the pressure it was exerting. Establishing and maintaining the reduction before temporary stabilization with a regular K wires was simplified ernormously through use of this retractor. My only comment is think carefully about the location of the retractor pins with respect to the position of the plate so that both don’t come into conflict when attempting to position the plate.
Orthopaedic implants used: DePuy Synthes Variable Angle LCP Two-Column Volar Distal Radius Plate 2.4
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1576 times
15 Mar 2021
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2021). Reverse Barton's fracture 2R3B3.1. Journal of Orthopaedic Surgery and Traumatology. Case Report 8371242 Published Online Mar 15 2021.