














Hyperextension Plateau Depression with PLC Avulsion
Score and Comment on this Case
Clinical Details
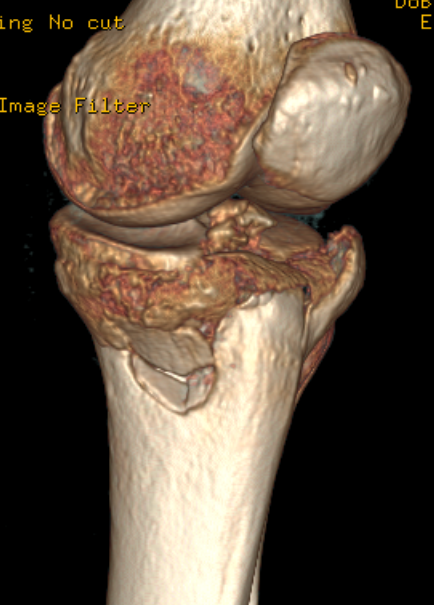
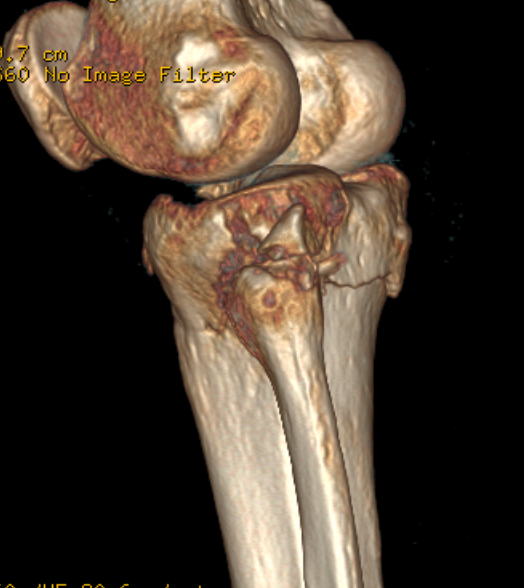
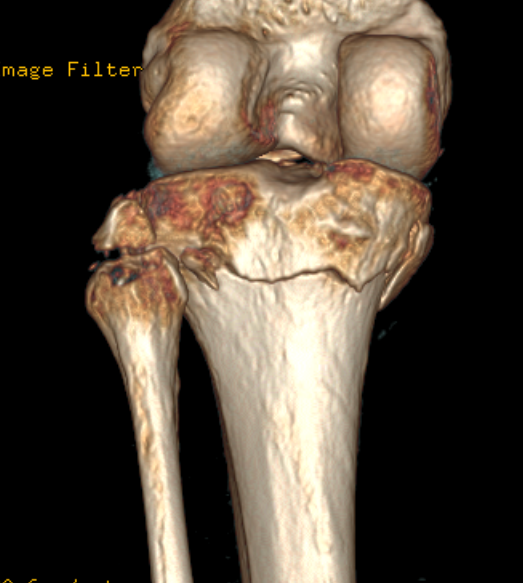
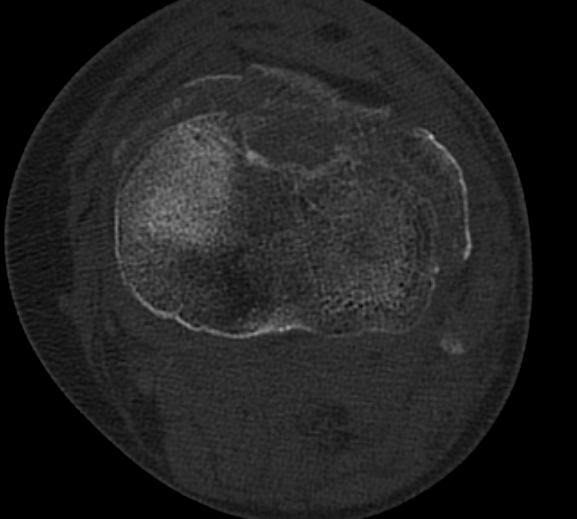
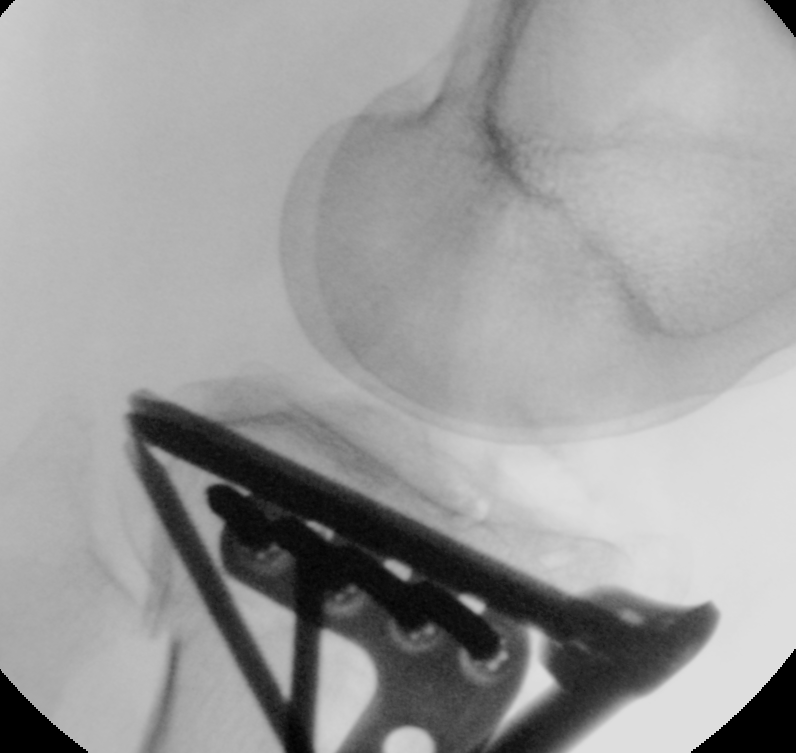
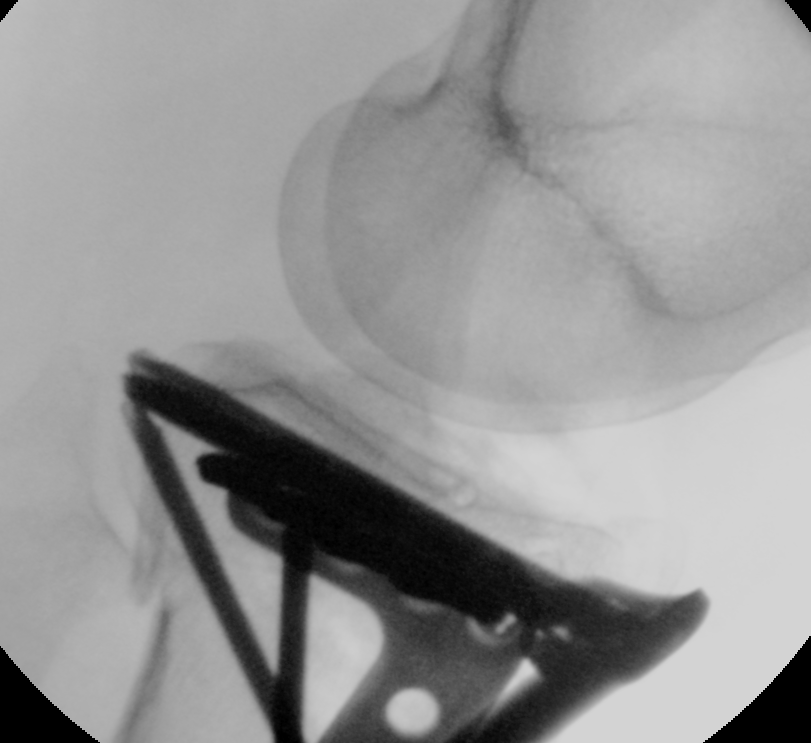
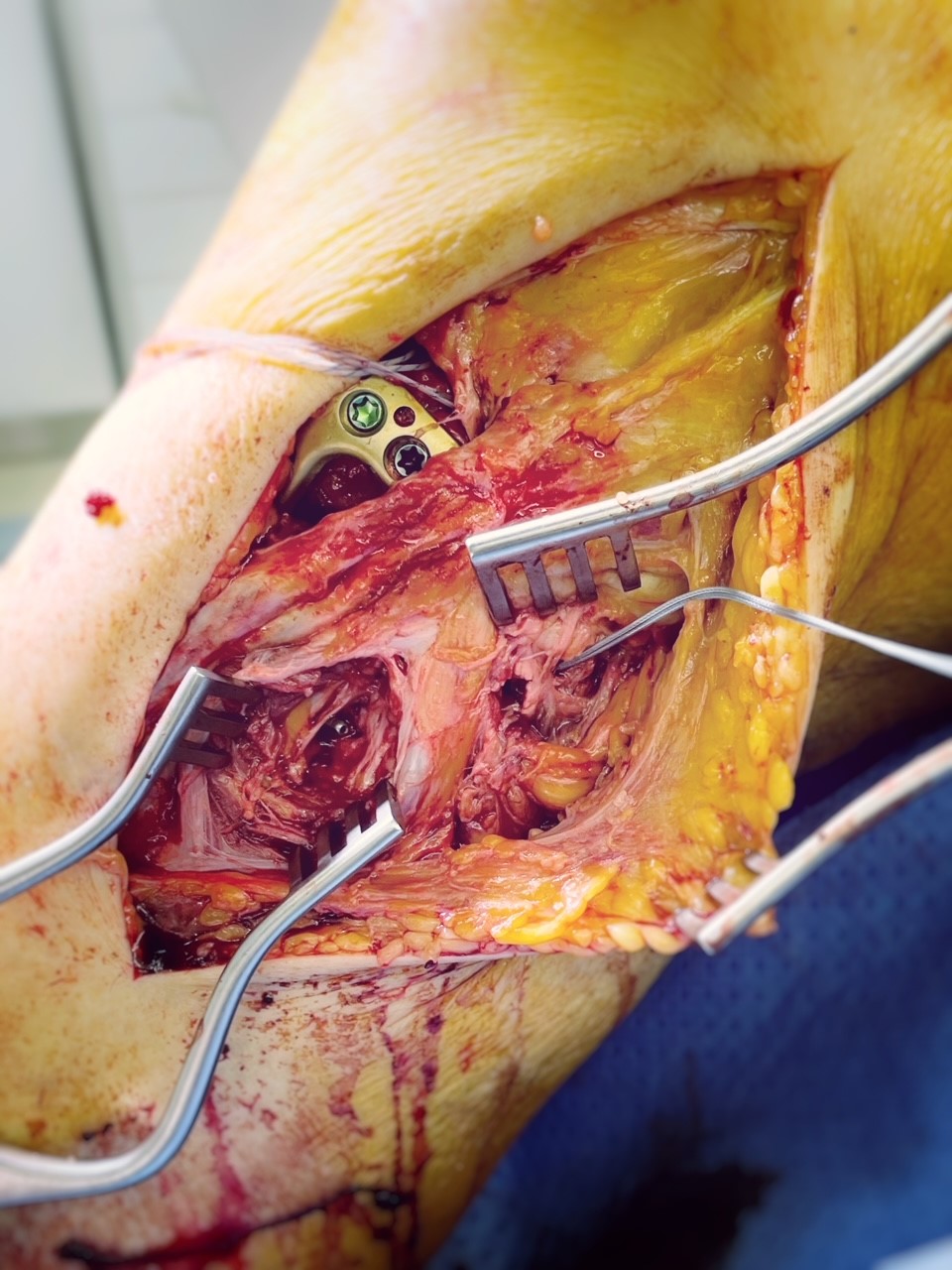
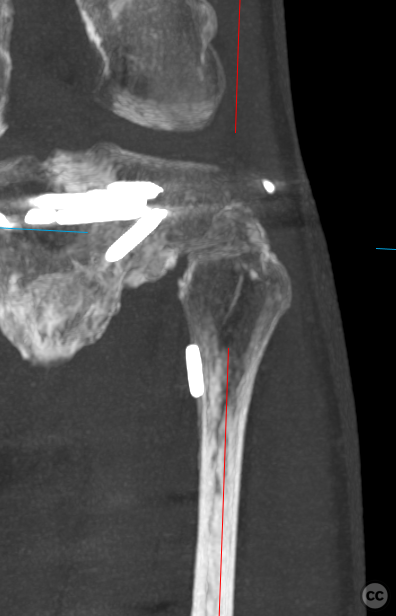
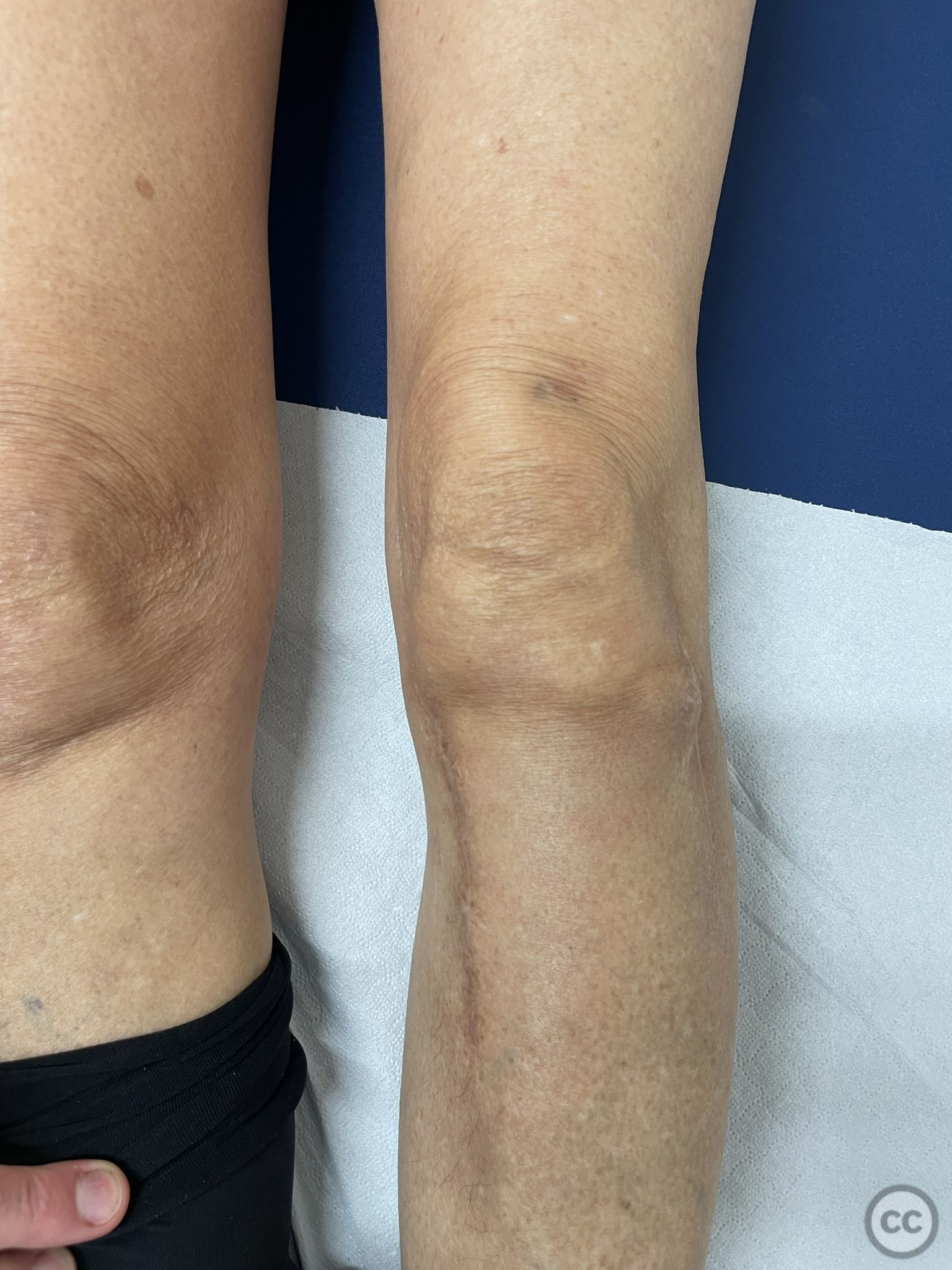
Clinical and radiological findings: This case is a hyperextension injury of the left knee with anterior impaction of the medial and lateral tibial plateau articular surfaces. The degree of impaction is more pronounced medially tending into varus, though a significant loss of overall height of both condyles is evident. In addition we note the avulsion fracture of the tip of the proximal fibula implying avulsive disruption of the posterolateral corner ligament complex including the arcuate ligament and the popliteaofibular ligament. As can be seen in the preoperative clinical photos the knee falls into marked hyper extension and varus with posterolateral laxity. The surgical approach began mediately with an initial elevation and reconstruction of the medial joint height. This was unable to be restored in isolation so following provision plate placement and fixation of medial height with k-wires we opened the lateral approach, then moving between medial and lateral sides the entire joint surface could be sequentially elevated en-block. An intra-operative shot of the contralateral uninjured side provided a guide to the inclination of the tibial articular slope and using this as a guide we reconstructed both articular height and tibial slope to comparable pre-injury state. The fixation comprised of medial and lateral 3.5 mm anatomical locking plates. Following bony reconstruction clinical hyperextension was greatly reduced. A further consequence of restoring length of the lateral column was a spontaneous retentioning of the lateral collateral ligament. The disruption to the posterolateral corner however remained clinically evident with residual posterolateral rotatory instability. Addressing the fibula avulsion involved neurolysis and mobilisation of the common peroneal nerve in it's course posterior to the biceps tendon continuing laterally around the fibula neck. Following protection and mobilization of the nerve we then drilled anterograde for placement of a transosseous endobutton suture (Arthrex distal biceps repair system) and anchored the PLC ligament complex with the avulsion fracture.
Preoperative Plan
Planning remarks: plan
Surgical Discussion
Operative remarks:In comparison to a recent similar case of a tibial plateau fracture with concomitant proximal fibula fracture (a direct compression injury in which the fibula fracture was ultimately managed nonoperatively) the hyperextension nature of this injury and the avulsive rupture of the poster lateral corner resulted in a higher degree of Posterolateral instability and required surgical stabilization. The use of screw osteosynthesis or tension band wiring could be considered however given fragment size and previous success with endobutton tightrope fixation of these fragments this was our choice of reconstruction in this case.
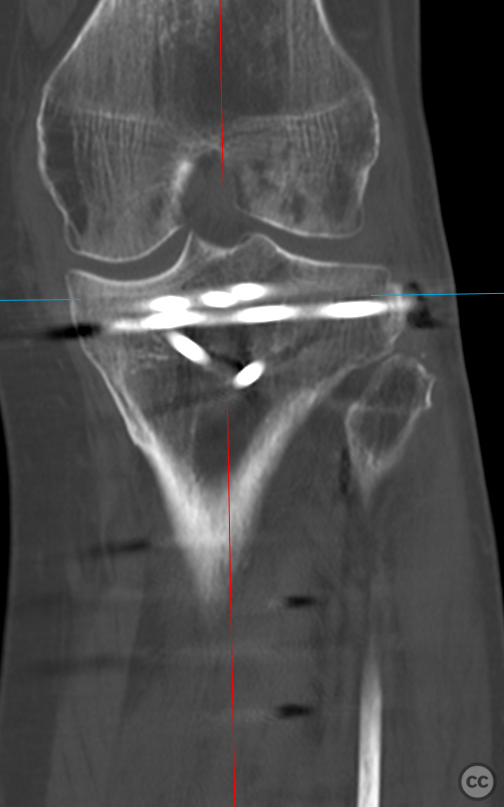
Postoperative protocol: Follow up images are at 18months. Full return to sports, no residual instability.
Orthopaedic implants used: DePuy Synthes 3.5mm medial and lateral proximal tibial plates. Arthrex distal biceps tendon repair system (endobutton delivery system)
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1331 times
13 May 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Hyperextension Plateau Depression with PLC Avulsion. Journal of Orthopaedic Surgery and Traumatology. Case Report 8413791 Published Online May 13 2022.